Myopia
Why control myopia?
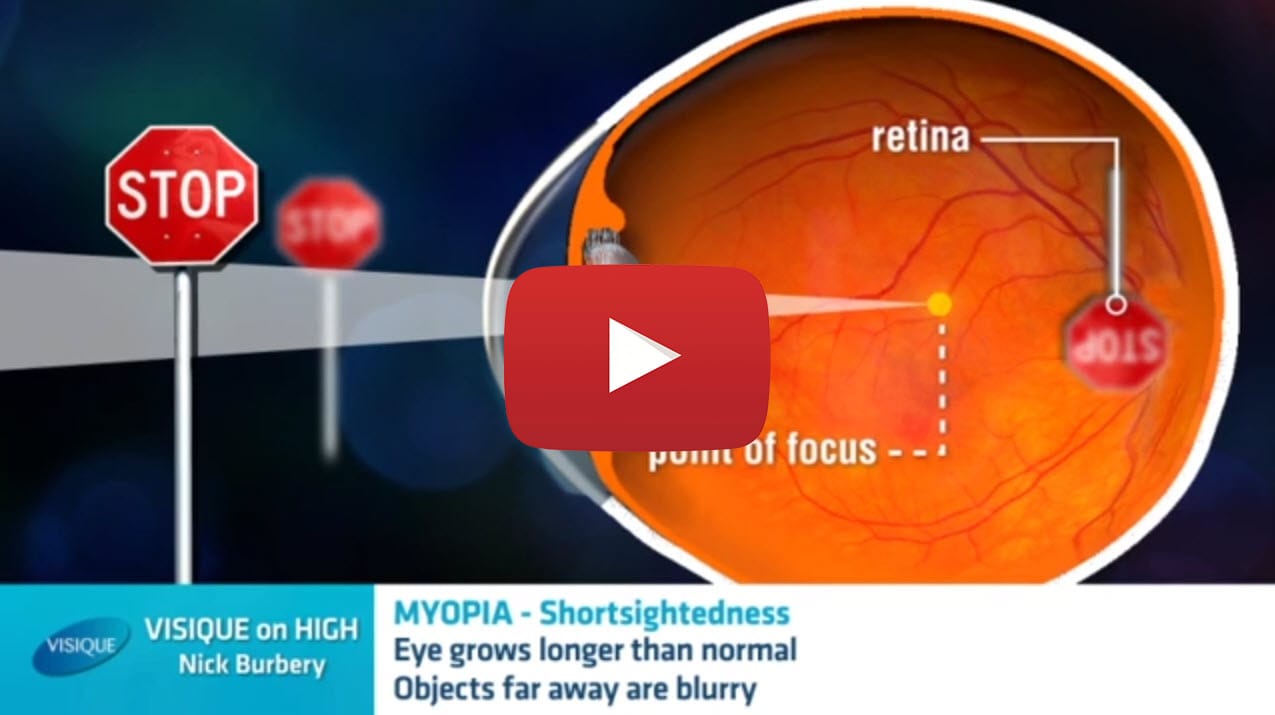
Myopia — or short-sightedness — refers to poor distance vision but clear near vision. This occurs when the eyeball grows too long in relation to the power of the eye’s lenses. The light rays then focus at a point in front of the retina, rather than directly on its surface.
The main reason to control myopia is the risk of blinding conditions that escalates as myopia increases.
Progression and associated risks
Adult-onset myopia (developing after 20 years of age) can progress over time, though youth-onset (before 20 years) generally shows more aggressive progression which continues until the eye stops growing. Typical sufferers are highly dependent on high-powered glasses or contact lenses and require frequent replacements as the condition escalates.
Myopia usually appears in childhood. The condition does run in families with parents having myopia being the strongest risk factor for myopia; however, some children are becoming short-sighted even though their parents have no distance vision problems. Genetics are therefore not the only contributing factor.
All levels of myopia increase the chance of blinding conditions such as retinal detachment, cataracts, glaucoma and myopia retinal degeneration later in life.
This risk escalates as the level of myopia increases. Myopic maculopathy, a progressive condition causing holes in the retina due to overstretching, is the fourth most common cause of permanent visual impairment in the UK, ahead of diabetic eye disease.
Studies show the risk factor for eye disease due to myopia is comparable to the risk of cardiovascular disease due to untreated high blood pressure. The risk for glaucoma and cataract due to myopia compares to the risk of stroke from smoking over 20 cigarettes per day. For retinal detachment and myopic maculopathy, myopia carries a risk far more than any identified population risk factor for cardiovascular disease. Given that higher levels of myopia entail a higher risk of these conditions, halting this progression can broadly prevent a significant level of blindness.

A chart showing the increased risk of different eye disease with higher levels of short-sightedness. Courtesy of the OSO
Myopia prevalence
The increase in myopia cases is worryingly high. It has doubled in the last 30 years. The highest levels of myopia are in East and South-East Asia where 80-90% of school leavers are short-sighted, and 20% are highly myopic. In Australia, North America and Europe 25-50% of children are now myopic, New Zealand is unlikely to be any different. There are approximately 1.4 billion people worldwide with myopia, by 2050 over 50% of the world’s population is expected to have short-sightedness.
Studies have shown that 93% of 18-year-old girls in Taiwan are myopic. In Singapore, seven out of ten college graduates have the condition, and China is experiencing rates up to 78% among 15-year olds in urban areas. Closer to home in Australia, 30% of teenagers finishing school are myopic — and this percentage is on the rise – the prevalence among Australian 12-year-olds doubled between 2005 and 2011.
More than just genetics?
The development of myopia seems to also be influenced by environmental factors, such as time outdoors, device use and near work.
Several studies have shown not enough time outdoors has a conclusive role. The latest research to come out of Perth, Australia shows the risk of myopia is reduced by up to 50% if children were to increase outdoor time from one to three hours a day.
The more near work performed, the more likely your child will become short-sighted, as does too much time spent on devices such as ipads and smartphones. There are a number of studies, including a recent example, that demonstrates an association between myopia and smartphone data usage. What is not clear at this stage is the degree to which the close distance at which the smart phones are held is what causes or increases the myopia, or is it the smart phone itself? As for television? Not believed to be a significant factor if your child is at least two metres away. The bigger the screen – the further away they need to be.
Why haven’t I been told about myopia control before?
It’s a great question to ask your current eyecare provider, as there are a variety of reasons. They can vary, from a lack of awareness of myopia control effectiveness, to deciding that controlling myopia is too time consuming for their core business model.
At Visique, knowing what we know about myopia and what we can do to help your child, we consider it our duty of care that we offer you all the evidence-based options that are available today, so you can make the most informed decision for your child’s eyesight and long-term eye health.
What can be done?
At Visique we take a pro-active approach to controlling myopia progression.
Prescribing standard spectacle lenses or contact lenses for your child or teenager won’t do anything to slow the progression of short-sightedness. As a result, frequent changes to their glasses will be needed and they will be put at risk of sight-threatening problems in the future. Unfortunately, the lengthening of the eye which causes myopia cannot be reversed, making it critical to control myopia sooner rather than later.
The good news is that there is conclusive evidence that certain treatments can slow and even halt the progression of myopia.
At Visique we ensure we are up to date with the latest research in this area and we will recommend the most appropriate myopia control methods for your child or teenager, depending on a range of factors.